
Knee pain is one of those things people tend to push through. You take a painkiller, rest it over the weekend, and tell yourself it will ease off. Sometimes it does. But for millions of people across the UK, it keeps coming back — and slowly, quietly, it starts to shape the way you live.
You stop taking the stairs without a second thought. You hesitate before a long walk. You wake up in the morning and your first few steps feel like you are moving through concrete. If any of that sounds familiar, there is a strong chance knee osteoarthritis is part of what you are dealing with.
This article explains what knee osteoarthritis actually is, why it develops, how it is diagnosed, and — most importantly — what can genuinely be done about it. Including newer treatments that many patients have never been told exist.
What Is Knee Osteoarthritis?
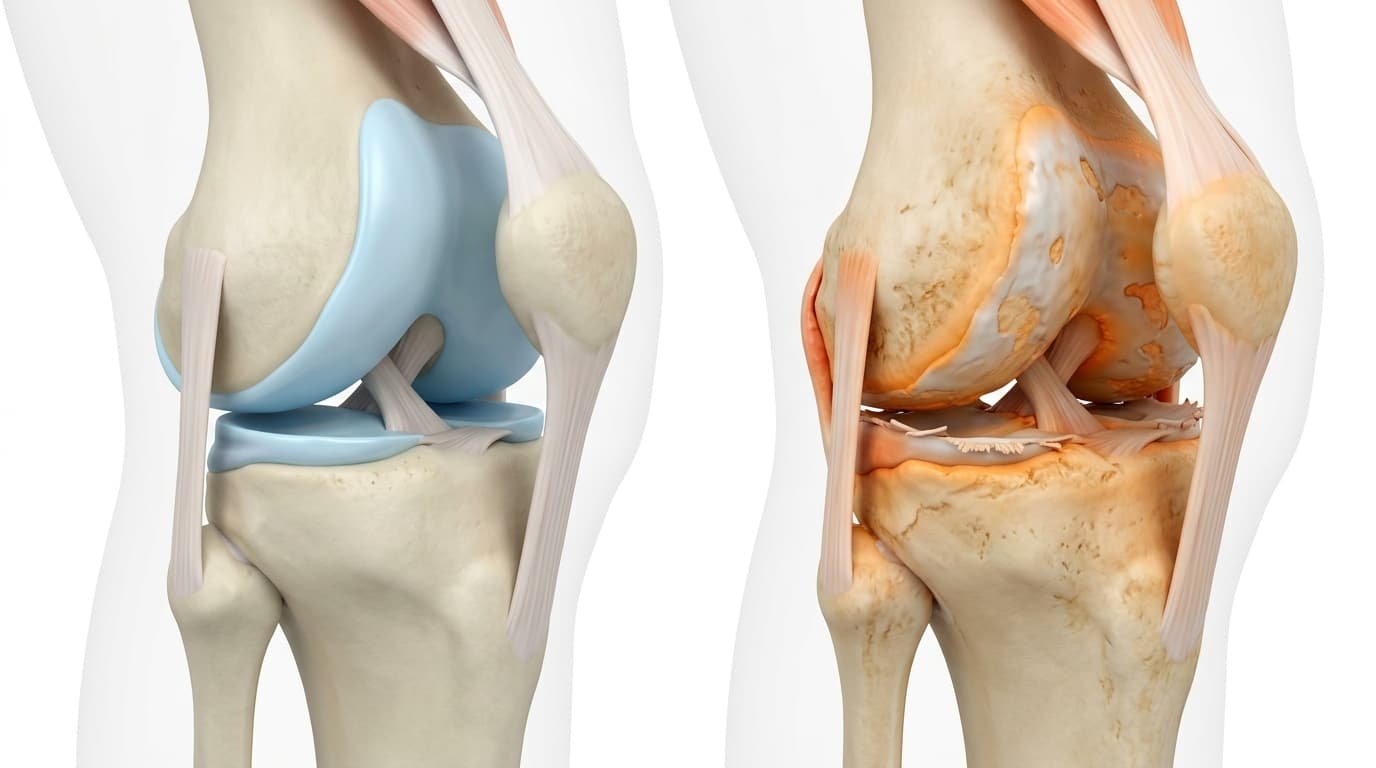
Knee osteoarthritis is a degenerative joint condition. It develops when the cartilage inside the knee — the smooth, rubbery tissue that cushions the joint and allows the bones to glide against each other — gradually breaks down over time.
As the cartilage thins, the bones begin to move with less protection. This causes friction, inflammation, pain, and stiffness. In more advanced cases, the cartilage wears away entirely, and the bones grind directly against each other. That is what clinicians mean when they use the phrase “bone on bone.”
Osteoarthritis is the most common form of arthritis in the UK. The knee is one of the most frequently affected joints — and for good reason. The knee absorbs a significant proportion of your body weight with every step you take. Over decades, that load accumulates.
It is worth noting something important: osteoarthritis is not simply the result of getting old. Age is a factor, but it is one of several. Understanding why osteoarthritis develops helps you take a more informed role in managing it.
What Causes Knee Osteoarthritis?
No single cause drives every case of knee osteoarthritis. In most people, several factors contribute simultaneously.
Age
The risk of developing knee osteoarthritis increases with age. The cartilage becomes less resilient over time, and the body’s capacity to repair and regenerate tissue slows down. Most people who develop knee osteoarthritis are over the age of 45, though younger people are certainly not immune — particularly those with a history of joint injury.
Body Weight
This is one of the most significant and most modifiable risk factors. The knee bears roughly three to four times your body weight when you walk, and up to six times when you climb stairs. Even modest excess weight places a substantially higher load on the joint over years and decades. Research shows that losing as little as five kilograms can meaningfully reduce knee pain in people with osteoarthritis.
Previous Knee Injury
A history of knee injury — ligament damage, a meniscal tear, a fracture involving the joint — significantly increases the risk of developing osteoarthritis in later life. The injury disrupts the mechanics of the joint, even after it heals. Over time, that disruption accelerates cartilage wear.
Gender
Women are disproportionately affected by knee osteoarthritis. They develop it more often than men, tend to experience it more severely, and often notice the onset at an earlier age. Hormonal changes around the menopause are a key driver. Oestrogen plays a protective role in cartilage health. When oestrogen levels fall significantly after the menopause, that protection reduces — and many women notice a clear worsening of knee symptoms in their 50s.
Women also have a wider pelvis than men, which creates a greater angle between the hip and the knee. This Q-angle, as it is known clinically, places more lateral stress on the joint with every step.
Genetics
Osteoarthritis runs in families. If a parent or sibling has it, your own risk is higher. Certain genetic factors affect the quality and resilience of cartilage, as well as the shape of the joint itself.
Occupation and Activity
Jobs and activities that involve repeated kneeling, squatting, heavy lifting, or prolonged standing increase the wear and tear on the knee joint over time. Manual workers, athletes, and those in physically demanding roles carry a higher lifetime risk.
Recognising the Symptoms of Knee Osteoarthritis
Knee osteoarthritis does not arrive with a single dramatic moment. It tends to develop gradually — which is one of the reasons people often dismiss the early signs or attribute them to something else.
The most common symptoms include:
- Pain in or around the knee that worsens with activity and improves with rest — until eventually it is present even at rest
- Stiffness in the morning or after sitting for a prolonged period, which typically loosens after a few minutes of movement
- A creaking, grinding, or clicking sensation when bending or straightening the knee — clinically referred to as crepitus
- Swelling around the knee, which may come and go, often worse after activity
- Reduced range of movement — difficulty bending or fully straightening the knee
- A feeling of weakness or instability, as though the knee might give way
- Pain on the stairs, getting in and out of a car, rising from a low chair, or walking on uneven ground
One of the things that surprises many patients is how poorly their pain can correlate with what shows up on imaging. A scan might show relatively mild structural changes — yet the pain is severe. Or conversely, the scan might show significant wear — but the symptoms are manageable. This is because osteoarthritis pain is not driven by structural damage alone. Inflammation of the synovial membrane — the soft lining inside the joint — plays an equally important role in generating pain. Understanding this changes how you approach treatment.
How Is Knee Osteoarthritis Diagnosed?

A proper diagnosis involves more than looking at a scan. A thorough clinical assessment is essential.
Mr S N Abbas will take a full history of your symptoms — when the pain started, what makes it better or worse, how it affects your daily life — and carry out a physical examination of the joint. He assesses the range of movement, the degree of swelling, the alignment of the knee, and the pattern of tenderness.
Imaging supports the clinical picture — it does not replace it. X-rays remain the standard first-line imaging for osteoarthritis. They can show joint space narrowing, bone spurs (osteophytes), and changes in the bone beneath the cartilage. An MRI is sometimes requested to provide a more detailed view of the soft tissues — the cartilage, the menisci, and the synovial membrane.
The combination of a clinical assessment and appropriate imaging allows Mr Abbas to confirm the diagnosis, gauge the severity, and recommend the most suitable treatment pathway for your specific situation.
Treatment Options for Knee Osteoarthritis
There is no cure for osteoarthritis — the cartilage does not regenerate. But that does not mean you are simply left to manage it indefinitely with painkillers. A great deal can be done to reduce pain, improve function, and maintain quality of life.
Treatment generally follows a stepped approach, from the simplest and least invasive options through to more advanced interventions.
Lifestyle Modifications
This is always the starting point. Weight management, low-impact exercise — swimming, cycling, walking at a comfortable pace — and activity modification can make a significant difference in the early stages. Strengthening the muscles around the knee, particularly the quadriceps, helps to protect the joint and reduce the load it absorbs.
Physiotherapy
A structured physiotherapy programme is one of the most effective tools available for managing knee osteoarthritis. Targeted exercises strengthen the muscles that support the knee, improve proprioception, and can meaningfully reduce pain over time. Physiotherapy works best when it is consistent and progressive.
Medication
For mild to moderate pain, paracetamol remains the first-line recommendation from NICE. Topical anti-inflammatory gels — such as diclofenac applied directly to the knee — are often helpful and carry fewer systemic risks than oral anti-inflammatory tablets. Oral NSAIDs such as ibuprofen or naproxen provide more significant relief but should be used cautiously, particularly in older patients.
None of these options address the underlying joint condition. They manage symptoms.
Steroid Injections
A corticosteroid injection into the knee can reduce inflammation and provide meaningful pain relief — often within days. The effect typically lasts between six and twelve weeks. Steroid injections are useful for acute flare-ups and for getting pain under control before starting physiotherapy. They are not a long-term solution. Repeated use can damage cartilage over time.
Hyaluronic Acid Injections
Hyaluronic acid injections were widely used for knee osteoarthritis for many years. NICE no longer recommends them as part of routine osteoarthritis management, following a review of the evidence base. Their use has declined significantly in recent years.
Arthrosamid Injection — A Newer Approach to Knee Osteoarthritis
For patients who have tried conservative treatments and are not yet ready for surgery, Arthrosamid injection represents one of the most significant advances in knee osteoarthritis management in recent years.
What Is Arthrosamid?
Arthrosamid is a non-biodegradable hydrogel. It is made of 97.5% water and 2.5% cross-linked polyacrylamide. It is injected directly into the knee joint under ultrasound guidance — a precision procedure that requires an experienced clinician.
Once inside the joint, the hydrogel gradually integrates with the synovial membrane — the soft tissue lining the inside of the joint. Over four to six weeks, it becomes part of the joint environment. This integration is believed to increase the elasticity and resilience of the synovial tissue, reduce inflammation, and improve the overall mechanical environment within the knee.
Because it is non-biodegradable, Arthrosamid does not break down the way other injectable treatments do. It remains active within the joint rather than being reabsorbed over weeks or months.
What Does the Evidence Say?
Clinical studies on Arthrosamid have shown sustained improvements in pain and function. A published five-year follow-up study reported continued, meaningful improvements at that time point — a result that no other non-surgical injectable treatment has matched in clinical data.
For patients with mild to moderate knee osteoarthritis whose symptoms persist despite physiotherapy, medication, and other conservative measures, Arthrosamid offers a genuine, evidence-backed option that may significantly delay or avoid the need for knee replacement surgery.
How Is Arthrosamid Different From a Steroid Injection?
A steroid injection reduces inflammation temporarily — the effect typically fades within weeks to months. Arthrosamid works differently. It does not simply dampen inflammation; it physically integrates with the synovial tissue and supports the joint environment over a much longer timeframe. It is a fundamentally different mechanism, not a more powerful version of the same thing.
Is Arthrosamid Right for You?
Arthrosamid tends to be most suitable for patients with mild to moderate knee osteoarthritis who have persistent symptoms despite conservative treatment and who are not yet at a stage where knee replacement is the only remaining option.
It is generally not suitable for patients with very advanced (bone-on-bone) osteoarthritis, active knee infection, or allergy to polyacrylamide.
The only way to confirm suitability is a face-to-face consultation. At Dr SNA Clinic, Mr Abbas performs every Arthrosamid injection personally — with ultrasound guidance, a dual-spin centrifuge protocol, and full post-injection support as standard.
When Is Knee Replacement Surgery Considered?
Knee replacement surgery — total or partial — remains a reliable and effective option for patients with advanced knee osteoarthritis where conservative treatments no longer provide adequate relief.
It is typically considered when:
- Pain is severe and persistent, significantly affecting quality of life
- Daily activities such as walking, sleeping, and dressing are substantially impaired
- Conservative treatments have been exhausted and failed to provide adequate benefit
- Imaging confirms advanced joint deterioration
Modern knee replacement surgery has excellent long-term outcomes. Most patients experience significant pain relief and improved mobility. Implants typically last fifteen to twenty years.
That said, surgery carries risks — infection, blood clots, anaesthetic complications, and a recovery period of several months. For many patients, the goal is to delay that decision for as long as possible while maintaining a reasonable quality of life. That is precisely where treatments like Arthrosamid play their role.
Living With Knee Osteoarthritis — Practical Steps

Managing knee osteoarthritis well is an active process. There are genuine things you can do every day that influence how the condition progresses and how much it affects your life.
Keep moving. It sounds counterintuitive when movement causes pain, but inactivity weakens the muscles around the joint and allows stiffness to worsen. Low-impact activity — swimming, cycling, walking — keeps the joint mobile and the surrounding muscles strong.
Manage your weight. Even a modest reduction in body weight reduces the load on the knee substantially over time. This is one of the highest-impact changes you can make.
Stay consistent with physiotherapy. The exercises need to be done regularly to work. Sporadic effort produces sporadic results.
Do not dismiss your symptoms. Many people live with significant knee pain for years before seeking an assessment. The earlier you address knee osteoarthritis, the more options are available to you. Waiting until the condition is advanced narrows the choices considerably.
Final Thoughts
Knee osteoarthritis is common, progressive, and — if left unmanaged — genuinely life-limiting. But it is not inevitable that it controls your life. With the right assessment, the right treatment plan, and the right clinician behind you, it is possible to reduce pain, restore confidence in movement, and maintain the quality of life you deserve.
If you have been managing knee pain for months or years and are wondering whether something more can be done, the honest answer is: quite possibly, yes. An assessment with Mr S N Abbas at Dr SNA Clinic will give you a clear picture of where your knee stands — and what the most appropriate next steps look like for your specific situation.
You do not have to simply live with it.
Mr S N Abbas is a London-based award-winning orthopaedic and management of knee conditions, including knee osteoarthritis, ligament tears, meniscal injury, and patellofemoral pain syndrome. He is based at 48 Wimpole Street, Marylebone, London W1G 8SF.
To book a consultation, call +44 7955 836986 or visit drsnaclinic.com/booking
Read More: What Is Polyacrylamide Hydrogel and Why Is It Used in Arthrosamid?








