
Your knee is one of the hardest-working joints in your body. Every time you climb stairs, stand up from a chair, or go for a walk, your knee absorbs force and keeps you moving. So when something goes wrong with it, you feel it — often immediately, and often constantly.
Knee pain is one of the most common reasons people visit a doctor in the UK. It affects people of every age, every fitness level, and every lifestyle. But not all knee pain is the same. The cause of your pain determines everything — the right diagnosis, the right treatment, and how likely you are to fully recover.
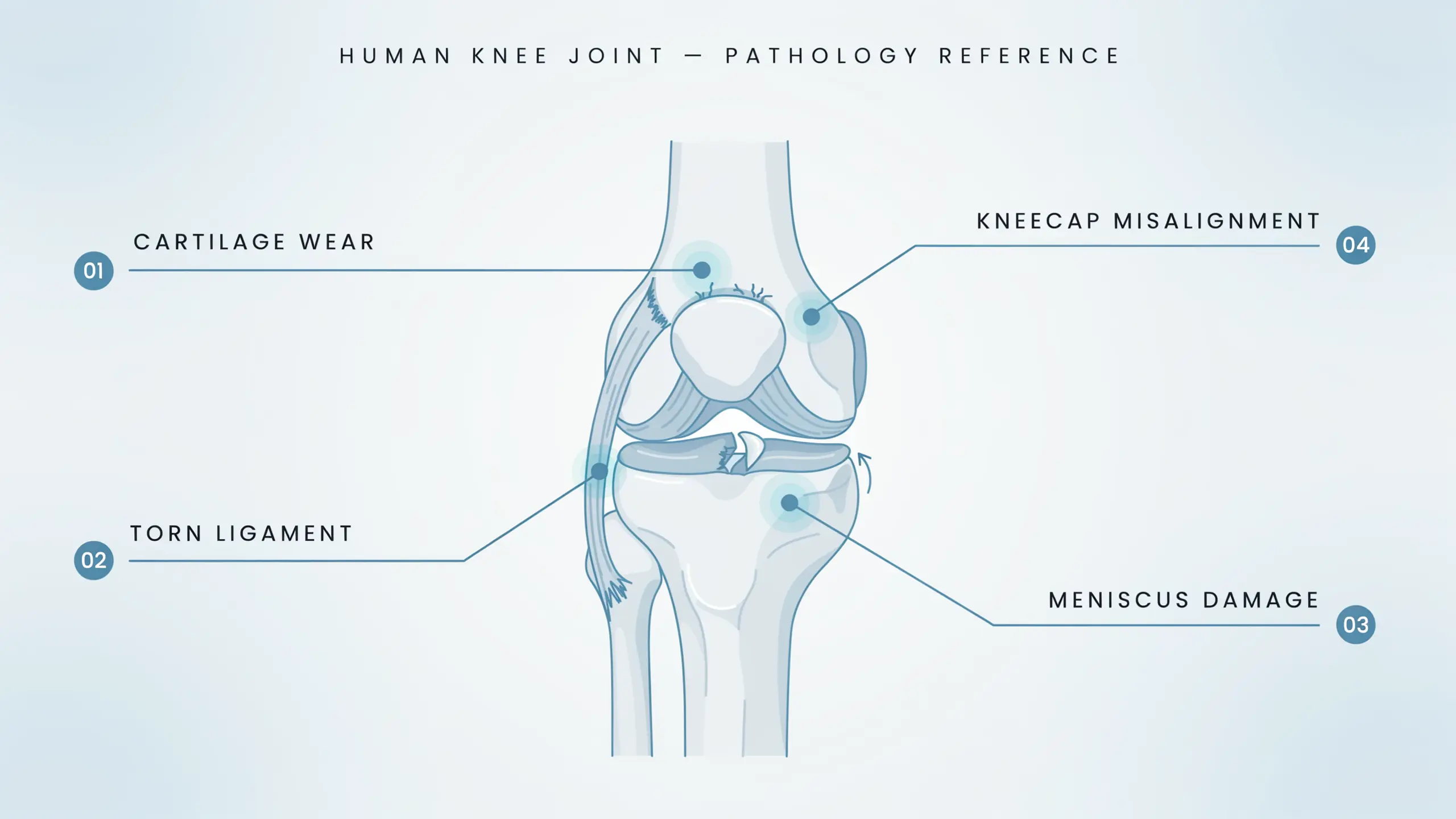
If you have been living with knee discomfort and wondering what is actually going on inside the joint, this guide will walk you through the four causes that account for the vast majority of cases — clearly, honestly, and without unnecessary medical jargon.
We also have a detailed guide on pain in the knee — its causes, treatments, and when to seek help if you want a broader picture alongside this one.
Why Does Knee Pain Happen?
Before diving into the four causes, it helps to understand what makes the knee so vulnerable in the first place.
The knee is not a simple hinge. It is a complex structure involving bones, cartilage, ligaments, tendons, and a fluid-filled joint capsule — all working together under significant mechanical load. When any one of those components becomes damaged, worn, inflamed, or misaligned, pain follows.
The good news is that most knee pain has a specific, identifiable cause. And once you know the cause, you have options.
Here are the four most common ones.
1. Osteoarthritis — The Gradual Wear of Cartilage
Osteoarthritis is the most common cause of knee pain in adults over 50. It is also one of the most misunderstood — because it develops slowly and quietly before the pain becomes impossible to ignore.
What Actually Happens
Inside a healthy knee, the ends of the bones are covered by a smooth layer of cartilage. This cartilage acts as a cushion and a gliding surface. It absorbs impact and allows the joint to move freely without friction.
In osteoarthritis, that cartilage gradually breaks down. It thins, softens, and eventually wears away in patches. As the protective layer disappears, bone begins to rub against bone. The joint becomes inflamed. Movement becomes painful. Stiffness sets in.This is not a process that happens overnight. It often develops over years or decades — which is why many people are surprised by how significant the damage already is when they finally get an X-ray.
Who Gets It
Osteoarthritis of the knee is more common in:
- Adults over 50
- Women — particularly after the menopause, when oestrogen levels fall and cartilage loses some of its natural protection
- People who are overweight — every additional kilogram of body weight adds roughly four kilograms of force through the knee joint
- People with a history of knee injuries
- Those who have had physically demanding jobs or sports careers
What It Feels Like
The hallmark of knee osteoarthritis is a deep, aching pain that worsens with activity and eases with rest — at least in the earlier stages. As the condition progresses, the pain often becomes more constant.
Other common signs include:
- Morning stiffness that lasts 15 to 30 minutes before the joint loosens up
- A creaking or grinding sensation (known as crepitus) when you move the knee
- Swelling around the joint, particularly after activity
- Difficulty with stairs, getting in and out of a car, or rising from a low seat
- The knee gradually feeling less stable than it used to
What Helps
Osteoarthritis cannot be reversed, but it can absolutely be managed — and for many people, managed very well. Treatment options range from physiotherapy and weight management at one end to joint replacement surgery at the other.For patients whose symptoms persist despite conservative treatment, Arthrosamid injection is an option worth knowing about. It is a non-biodegradable hydrogel injected directly into the knee joint that integrates with the synovial tissue, reduces pain, and improves mobility. Clinical studies report sustained improvements for up to five years from a single injection. You can read more about the best ways to relieve knee pain in our dedicated guide.
2. Ligament Injuries — When the Knee’s Stabilisers Tear
Ligament injuries tend to happen suddenly and dramatically. Unlike the slow creep of osteoarthritis, a significant ligament injury usually announces itself with a loud pop, immediate swelling, and an alarming feeling that the knee can no longer hold you up.
What Actually Happens
Ligaments are the tough, fibrous bands of tissue that connect bone to bone and hold the knee joint together. The knee has four main ligaments:
- The anterior cruciate ligament (ACL) — runs diagonally through the centre of the knee and controls rotational stability
- The posterior cruciate ligament (PCL) — works with the ACL to control front-to-back movement
- The medial collateral ligament (MCL) — runs along the inner side of the knee
- The lateral collateral ligament (LCL) — runs along the outer side
The ACL is the most commonly injured of the four, particularly in sports that involve sudden changes of direction, jumping, or pivoting.
A ligament injury can range from a mild stretch (Grade 1) to a partial tear (Grade 2) to a complete rupture (Grade 3). Grade 3 tears are the most serious and often require surgical intervention to restore full stability.
Who Gets It
Ligament injuries are strongly associated with sport — particularly football, basketball, skiing, and rugby. However, they can also happen during everyday activities, especially in older adults with weakened supporting structures around the knee.
What It Feels Like
An ACL or MCL injury typically produces:
- A loud “pop” at the moment of injury — often heard or felt clearly
- Immediate, significant swelling — the joint can balloon within hours
- Instability — a feeling that the knee might give way or buckle
- Inability to bear weight on the affected leg
- Pain with any attempt to move the joint through its normal range
What Helps
Mild to moderate ligament sprains often heal with rest, physiotherapy, and graduated return to activity. More significant tears — particularly complete ACL ruptures in active individuals — frequently require surgical reconstruction followed by a period of intensive rehabilitation.
Early assessment is important. If your knee gave way, swelled rapidly, and has not felt right since, that warrants prompt clinical attention — not just a wait-and-see approach.
3. Meniscus Tears — The Shock Absorber Problem
The meniscus does not get the attention it deserves — until it tears, at which point it makes itself very well known.
What Actually Happens
Each knee has two menisci — the medial meniscus on the inner side and the lateral meniscus on the outer side. These are C-shaped pads of rubbery fibrocartilage that sit between the thighbone (femur) and shinbone (tibia). Their job is to distribute load evenly across the joint and act as shock absorbers.
Meniscus tears happen in two quite different ways. In younger people, they typically result from a forceful twisting or rotational movement — often during sport. In older adults, the meniscus becomes less resilient with age and can tear from relatively minor movements, or even from standing up awkwardly. The tear can vary in size and shape — from a small radial tear to a large bucket-handle tear where a flap of cartilage folds over on itself and blocks the joint.
Who Gets It
Anyone can tear a meniscus. It is one of the most common knee injuries seen in clinical practice, affecting both athletes and sedentary adults. The degenerative type, which happens without a clear injury event, is particularly common in middle-aged and older adults.
What It Feels Like
A meniscus tear typically produces:
- Sharp, localised pain on the inner or outer side of the knee, depending on which meniscus is affected
- Swelling that develops over hours rather than immediately (slower than a ligament injury)
- A catching or locking sensation — the knee gets “stuck” and cannot fully straighten or bend
- Pain when twisting, squatting, or kneeling
- Giving way in some cases, when the torn fragment interferes with normal joint mechanics
What Helps
Treatment depends on the type, size, and location of the tear, as well as the patient’s age and activity level. Small, stable tears in the outer zone of the meniscus — where blood supply is better — can sometimes heal with physiotherapy alone. Larger tears, or those causing locking or instability, are often treated with arthroscopic surgery.
For older adults with degenerative meniscus tears, the approach is usually more conservative. Many of these patients also have underlying osteoarthritis, and the management strategy focuses on overall joint health rather than the tear in isolation.
4. Patellofemoral Pain Syndrome — Runner’s Knee
Patellofemoral pain syndrome (PFPS) is the most common cause of knee pain in younger active people — particularly runners, cyclists, and those who spend long periods sitting with bent knees. It is often called runner’s knee, though you absolutely do not have to be a runner to develop it.
What Actually Happens
The patella — your kneecap — sits in a groove at the front of the femur (thighbone) and glides up and down as you bend and straighten your knee. In a healthy knee, it tracks smoothly through this groove.
In patellofemoral pain syndrome, the kneecap tracks improperly — usually shifted slightly to one side due to muscle imbalances, tight structures, or subtle anatomical differences in how the knee is aligned. This abnormal tracking creates friction and increased pressure on the cartilage behind the kneecap, causing pain.
It is not necessarily a structural injury in the same sense as a ligament tear or a meniscus tear. It is more of a mechanical imbalance — but the pain it produces can be severe and persistent if left unaddressed.
Who Gets It
PFPS is particularly common in:
- Runners — especially those who have recently increased their mileage or changed their training surface
- Cyclists — particularly with incorrect saddle height
- Women — due to a wider pelvis, which creates a greater inward angle at the knee (the Q-angle) and increases the tendency for the kneecap to drift laterally
- People with tight IT bands, hip flexors, or calves
- Those who have recently taken up exercise after a period of inactivity
What It Feels Like
The symptoms of runner’s knee are quite distinctive:
- A dull, aching pain at the front of the knee or around the kneecap — not a sharp injury pain, but a persistent background ache that gets worse with certain activities
- Pain on stairs — particularly going downstairs, which places high load on the patellofemoral joint
- Pain after prolonged sitting with the knees bent — sometimes called the “theatre sign” because it was classically noted in people sitting through long films
- Pain when squatting or kneeling
- A grinding sensation when the knee moves
What Helps
The good news about PFPS is that it generally responds well to the right physiotherapy. Strengthening the quadriceps — particularly the VMO (vastus medialis oblique) on the inner side of the thigh — along with hip strengthening, often produces significant improvement over six to eight weeks.
Other helpful measures include temporary activity modification, taping techniques, appropriate footwear, and in some cases, orthotics. Steroid injections are occasionally used for acute flare-ups, though they address the inflammation rather than the underlying mechanical cause.
Surgery is rarely needed for PFPS.
How Do You Know Which One You Have?
Here is an honest answer: you often cannot tell with certainty without a proper clinical assessment.
The symptoms overlap more than most people expect. Pain on the inner side of the knee, for example, could indicate an MCL sprain, a medial meniscus tear, or medial compartment osteoarthritis — and the treatment for each is quite different. As a rough guide:
| Symptom Pattern | Most Likely Cause |
| Gradual onset, worse with activity, stiff in the morning, over 50 | Osteoarthritis |
| Sudden pop during sport, immediate swelling, instability | Ligament injury (ACL/MCL) |
| Twisting injury, locking or catching sensation, localised side pain | Meniscus tear |
| Front-of-knee ache, worse on stairs and after sitting, younger/active | PFPS (Runner’s Knee) |
This table is a starting point, not a diagnosis. If you are experiencing severe swelling, cannot bear weight, or feel that your knee might give way, see a clinician promptly. Do not wait and hope it resolves.
When Should You See a Specialist?
Some knee pain does settle with rest, simple analgesia, and time. But certain signs suggest you need professional assessment sooner rather than later:
- Significant swelling that developed quickly after an injury
- Inability to bear weight or straighten the knee fully
- A feeling of instability — the knee giving way or threatening to
- Locking — the knee getting stuck in one position
- Pain that has persisted for more than six weeks without improvement
- Night pain or pain at rest that is worsening
For chronic knee pain that has not responded to self-management and physiotherapy, it is worth exploring what options exist beyond standard NHS pathways. Our guide on how to stop knee pain covers every treatment option from conservative to advanced — including what the evidence says about each.
Frequently Asked Questions
Can I have more than one cause of knee pain at once?
Yes — and it is quite common, particularly in older adults. Someone might have underlying osteoarthritis and then develop a meniscus tear on top of it. Or a runner with PFPS might also have some early cartilage wear. This is one reason proper assessment matters: the treatment plan needs to address what is actually present, not just the most obvious symptom.
Is it safe to exercise with knee pain?
It depends on the cause. For osteoarthritis and PFPS, low-impact exercise — swimming, cycling, walking on flat ground — is generally beneficial and encouraged. For acute ligament injuries or significant meniscus tears, activity needs to be modified based on clinical advice. As a general rule, exercise that worsens your pain significantly or causes swelling the next day is telling you something worth listening to.
Will my knee pain go away on its own?
Some mild knee pain does resolve without treatment, particularly if it followed a single overuse episode. But pain that has been present for weeks or months rarely disappears without some form of intervention. The earlier you address it, the more options you have — and the better your long-term joint health tends to be.
What is the fastest way to reduce knee pain?
For acute pain and swelling: rest, ice (wrapped in a cloth, not directly on skin), and paracetamol as a first step. Elevation can also help with swelling. For more persistent pain, physiotherapy addressing the underlying mechanical cause is the most effective long-term approach. If you are looking for a broader answer, our blog on what is the best way to relieve knee pain covers this in detail.
Is knee replacement the only option for severe osteoarthritis?
Not necessarily. For patients with persistent pain who are not yet ready for surgery — or who want to delay it — there are now advanced injectable treatments available privately. Arthrosamid, for example, is a non-biodegradable hydrogel injection that integrates with the synovial tissue inside the knee. Clinical studies report sustained pain relief for up to five years from a single treatment. It is not suitable for every patient, but for the right candidate, it represents a meaningful step between conservative management and surgery.
The Bottom Line
The four causes of knee pain — osteoarthritis, ligament injuries, meniscus tears, and patellofemoral pain syndrome — account for the large majority of cases seen in clinical practice. Each has a distinct mechanism, a distinct symptom pattern, and a distinct treatment pathway.
Knowing which one you are dealing with is not just academically interesting. It is the essential first step toward actually getting better.
If you have been managing knee pain quietly for weeks or months, the most useful thing you can do today is get a proper assessment from someone who will take the time to understand what is actually going on in your joint — and give you honest advice about what to do next.
Medically reviewed by Mr S N Abbas, MBBS, MRCSEd — Consultant in Orthopaedics and Regenerative Medicine, Dr SNA Clinic, 48 Wimpole Street, London. Updated June 2026.








